
The Complete Guide to the AIP Diet: What It Is, What the Research Shows, and How to Use It
If you work with clients managing autoimmune conditions, you’ve almost certainly been asked about the AIP diet. Some practitioners dismiss it as too restrictive. Others recommend it without fully understanding the clinical evidence behind it.
The reality sits somewhere more useful than either extreme. AIP has genuine clinical support for specific conditions, a clear mechanistic rationale, and a reintroduction framework that makes it meaningfully different from other elimination diets. It also has real limitations that are worth being honest about.
This guide covers everything you need to know — from the science behind why it works, to the food lists, to the clinical trial data, to practical guidance for clients navigating it day to day.
What Is the AIP Diet?
The Autoimmune Protocol diet was developed by Dr. Sarah Ballantyne as an extension of the Paleo diet, specifically designed for people with autoimmune conditions. The core premise: many modern foods contribute to intestinal permeability (“leaky gut”), dysregulated gut microbiome, and immune system dysregulation — all of which can worsen autoimmune symptoms.
AIP works in two phases:
- Elimination phase (30–90 days): Remove all foods that may trigger immune activation or damage the gut lining. The goal is to reduce baseline inflammation and let the gut heal.
- Reintroduction phase: Systematically add foods back, one at a time, over 5–7 days each, to identify which specific foods trigger symptoms for that individual.
The reintroduction phase is what separates AIP from other elimination diets. The goal isn’t permanent restriction — it’s building a personalized long-term diet based on data from your own body’s responses.
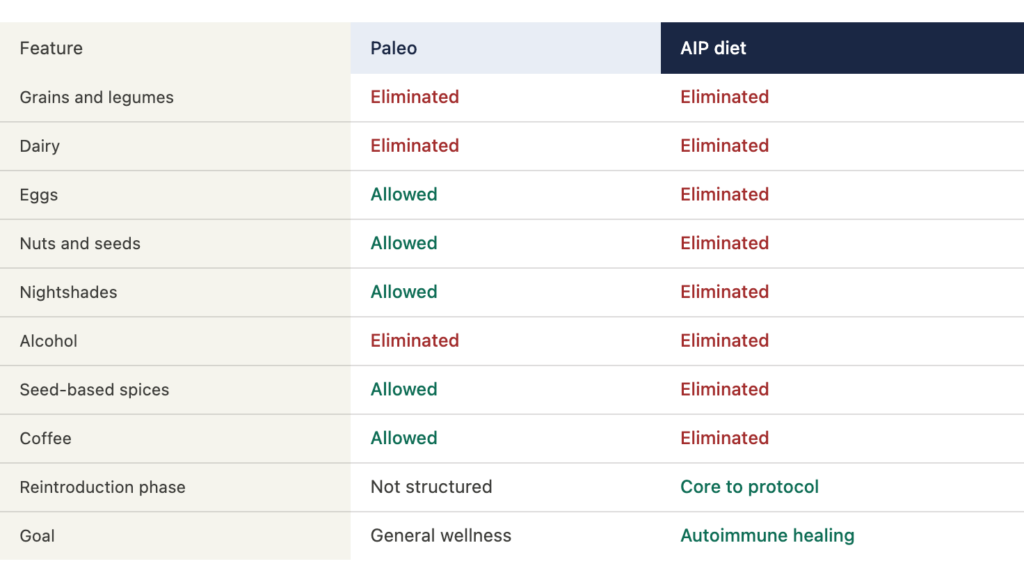
| AIP VS. PALEO — THE KEY DIFFERENCES People often confuse AIP with Paleo. They share a foundation but AIP goes significantly further in the elimination phase. |
| Feature | AIP diet |
| Grains and legumes | Eliminated |
| Dairy | Eliminated |
| Eggs | Eliminated (Paleo allows) |
| Nuts and seeds | Eliminated (Paleo allows) |
| Nightshades | Eliminated (Paleo allows) |
| Alcohol | Eliminated |
| NSAIDs | Avoided |
| Reintroduction phase | Core to the protocol |
| Goal | Autoimmune healing + personalization |
Why AIP Works: The Mechanism
AIP targets three overlapping problems that drive autoimmune flare-ups:
1. Intestinal permeability
The gut lining is a single-cell layer that acts as a selective barrier. When that barrier is compromised — by foods containing lectins, saponins, gluten, or certain gut-disrupting compounds — larger molecules including undigested food particles and bacterial endotoxins can pass through into the bloodstream, triggering immune responses.
AIP eliminates the foods most strongly associated with this process: gluten and grains, legumes (lectin-rich), nightshades (saponin content), dairy, and eggs. It also emphasizes foods that support gut lining repair: collagen-rich bone broth, omega-3 fatty acids, fermented foods, and a wide variety of plant-based fiber.
2. Gut microbiome disruption
Autoimmune conditions are consistently associated with reduced microbiome diversity and specific bacterial imbalances. AIP’s emphasis on vegetable diversity, prebiotic fiber, and fermented foods actively supports microbiome restoration. The elimination of processed foods, alcohol, and gut-disrupting ingredients removes ongoing insults to the microbiome.
3. Nutrient density
Many autoimmune clients are depleted in key nutrients that support immune regulation: vitamin D, zinc, selenium, magnesium, B12, and omega-3 fatty acids. AIP’s food list is built around nutrient-dense whole foods that address these deficiencies — grass-fed meats, wild-caught fish, organ meats, leafy greens, and colorful vegetables.
| THE BOTTOM LINE ON MECHANISM AIP doesn’t “treat” autoimmunity. It removes the most common dietary drivers of gut permeability and immune activation, supports microbiome repair, and restores nutrient density — creating conditions in which the immune system can regulate itself more effectively. |
What the Clinical Research Actually Shows

The AIP evidence base is promising but limited — it’s important to be accurate about both parts of that sentence.
IBD (Crohn’s disease and ulcerative colitis)
The strongest clinical evidence for AIP comes from IBD. A completed Scripps Health trial (NCT03512327) enrolled 15 patients with active Crohn’s disease or ulcerative colitis. Over an 11-week intervention (6-week elimination phase, then maintenance), the protocol measured clinical remission, inflammatory biomarkers (CRP, fecal calprotectin), endoscopic scores, and mucosal gene expression.
Results: clinical remission was achieved in the majority of participants. Fecal calprotectin levels improved. Mucosal gene expression showed changes consistent with reduced intestinal inflammation — including downregulation of inflammatory pathway genes. A follow-up study found improvements in quality of life and beneficial gene expression changes in the gut lining.
A separate 2017 study (the origin of the often-cited “73%” figure) found that 73% of participants with IBD reported significant symptom relief after 6 weeks on AIP.
Hashimoto’s thyroiditis
A 10-week open-label pilot study in 17 women with Hashimoto’s thyroiditis found significant improvements in quality of life scores and clinical symptom burden (severity and impact on daily life). C-reactive protein values and white blood cell counts were lower post-intervention. Importantly: there were no statistically significant changes in thyroid antibody levels (TPO or TGA) or TSH.
What that means for your clients: AIP may improve how Hashimoto’s patients feel day to day, but it’s not likely to normalize thyroid function or antibody levels. Set expectations accordingly.
Rheumatoid arthritis
A small clinical study (n = 9) found improvements in pain, sleep, and fatigue in RA patients following AIP while maintaining their existing medications. Sample size limits conclusions, but the directional signal is consistent with the IBD and Hashimoto’s data.
| HONEST EVIDENCE SUMMARY Strong signal: IBD — clinical remission rates, biomarker improvement, mucosal healing data Moderate signal: Hashimoto’s — quality of life and symptom improvement; no thyroid function normalization Early signal: RA — pain, sleep, fatigue improvement; very small sample Limited data: Lupus, MS, psoriasis, PCOS — anecdotal and community evidence, no completed controlled trials |
AIP Food Lists: What’s In, What’s Out
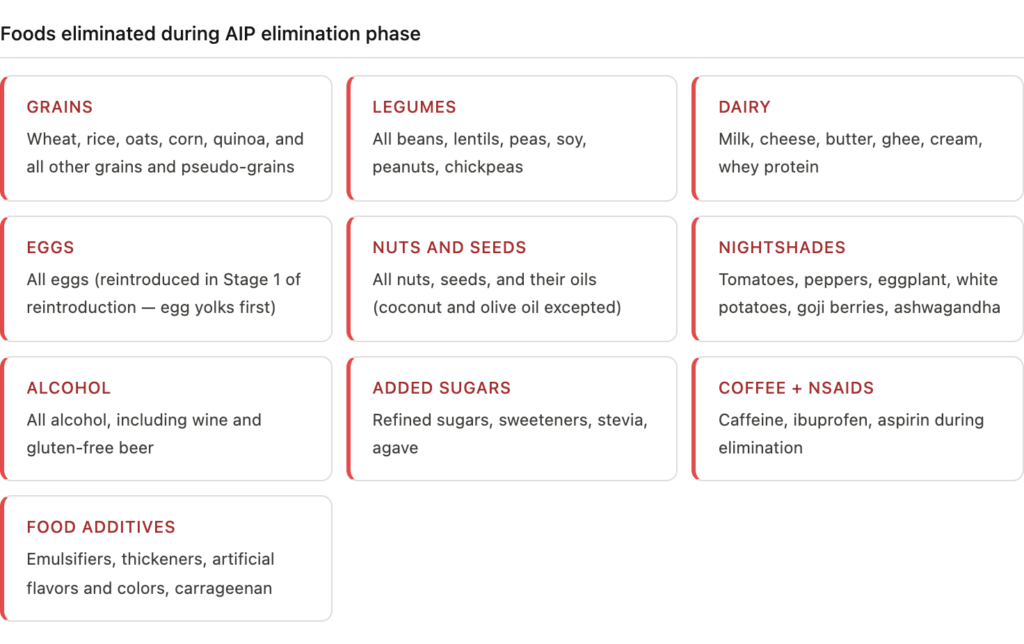
Foods eliminated on AIP
The elimination phase removes food groups associated with gut permeability and immune activation:
- Grains — wheat, rice, oats, corn, quinoa, and all other grains
- Legumes — all beans, lentils, peas, soy, peanuts
- Dairy — milk, cheese, butter, ghee, whey
- Eggs
- Nuts and seeds — including nut and seed oils (except coconut and olive)
- Nightshades — tomatoes, peppers, eggplant, potatoes, goji berries, ashwagandha
- Alcohol
- Refined/added sugars and sweeteners (including stevia)
- Food additives — emulsifiers, thickeners, artificial flavors, food colorings
- NSAIDs — ibuprofen and aspirin during elimination phase
- Coffee and caffeine
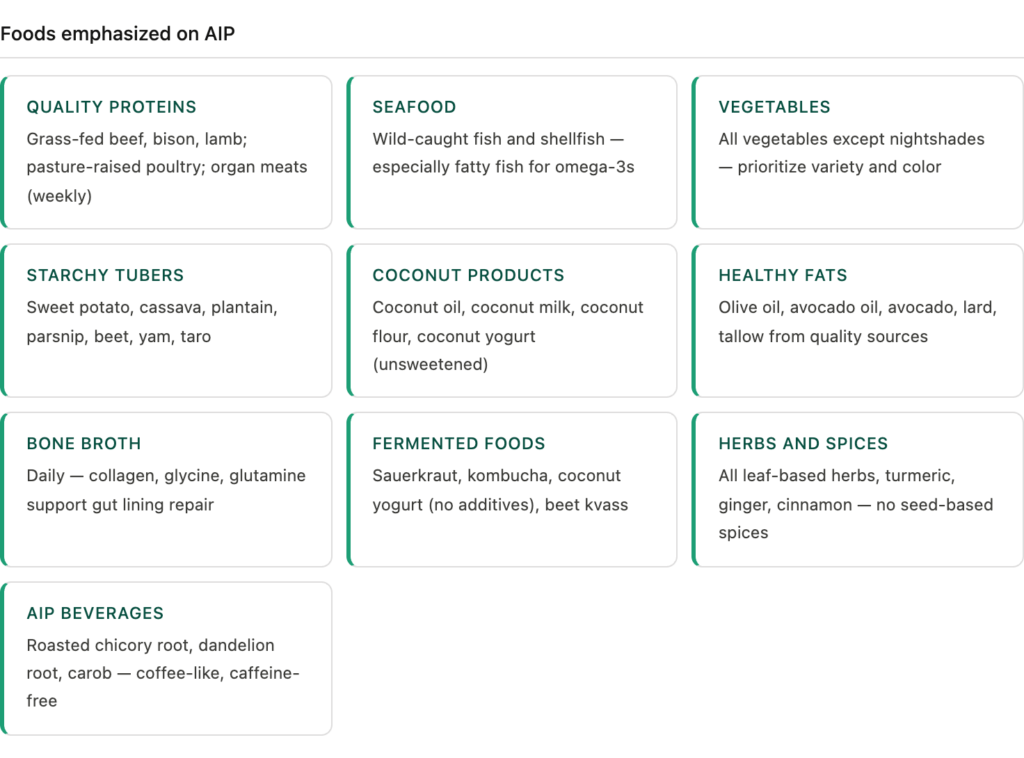
Foods emphasized on AIP
AIP is not just about removal. The foods emphasized are as important as the foods eliminated:
- Grass-fed, pasture-raised meats — beef, bison, lamb, pork, poultry
- Wild-caught fish and seafood — especially fatty fish for omega-3s
- Organ meats — liver, heart, kidney (nutrient-dense, encouraged weekly)
- Vegetables (all, except nightshades) — prioritize variety and color
- Tubers and starchy vegetables — sweet potato, cassava, plantain, parsnip, beet
- Fruit — in moderation
- Coconut products — coconut oil, coconut milk, coconut flour (unsweetened)
- Olive oil, avocado oil
- Bone broth — collagen and gut-lining support
- Fermented foods — sauerkraut, kombucha, coconut yogurt (without additives)
- Herbs and spices — all except seed-based (no cumin, coriander, caraway, fennel seed)
- Cassava flour — AIP-compliant baking staple
- Carob, chicory root, dandelion root — AIP-compliant beverage ingredients
The Two Phases: Elimination and Reintroduction
Phase 1: Elimination (30–90 days)
Most practitioners recommend a minimum of 30 days, with 60–90 days for clients with more severe or long-standing autoimmune conditions. The goal is to reach a sustained baseline of reduced symptoms before beginning reintroduction.
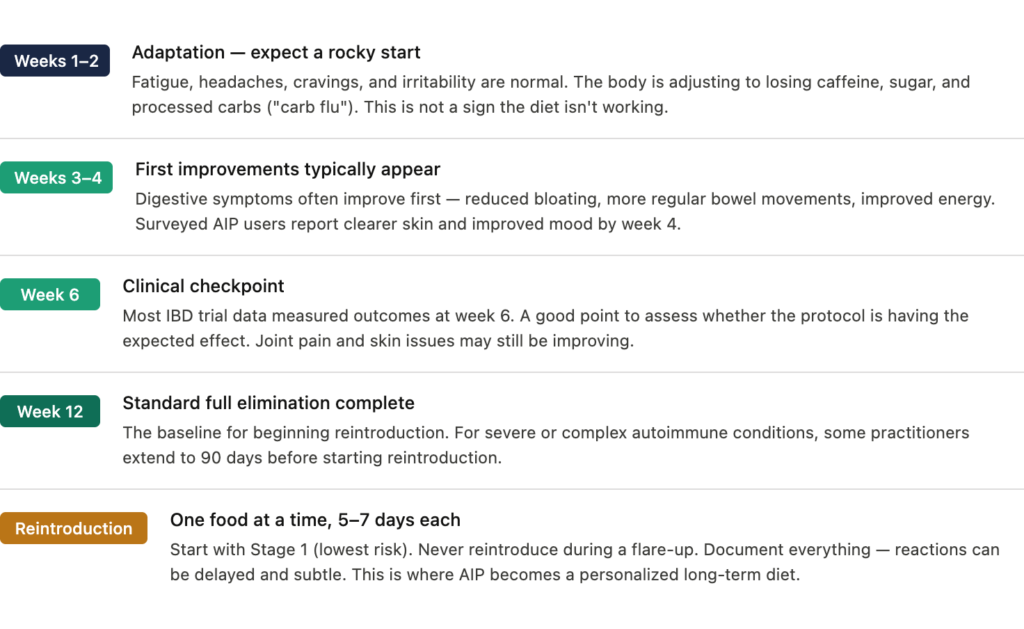
Common timeline:
- Weeks 1–2: adaptation symptoms — fatigue, headaches, cravings (“carb flu”). This is normal and temporary.
- Weeks 3–4: most clients notice digestive improvement, reduced bloating, better energy.
- Weeks 6+: the clinical checkpoint. Most IBD trial data measured outcomes at week 6.
- Week 12: standard full elimination before beginning reintroduction.
| CLIENT EXPECTATION MANAGEMENT The adaptation period (weeks 1–2) is the most common dropout point. Clients need to know in advance that fatigue, headaches, and irritability in the first two weeks are normal — not a sign the diet isn’t working. Meal prep and batch cooking before starting significantly reduce dropout. |
Phase 2: Reintroduction (the part most people skip)
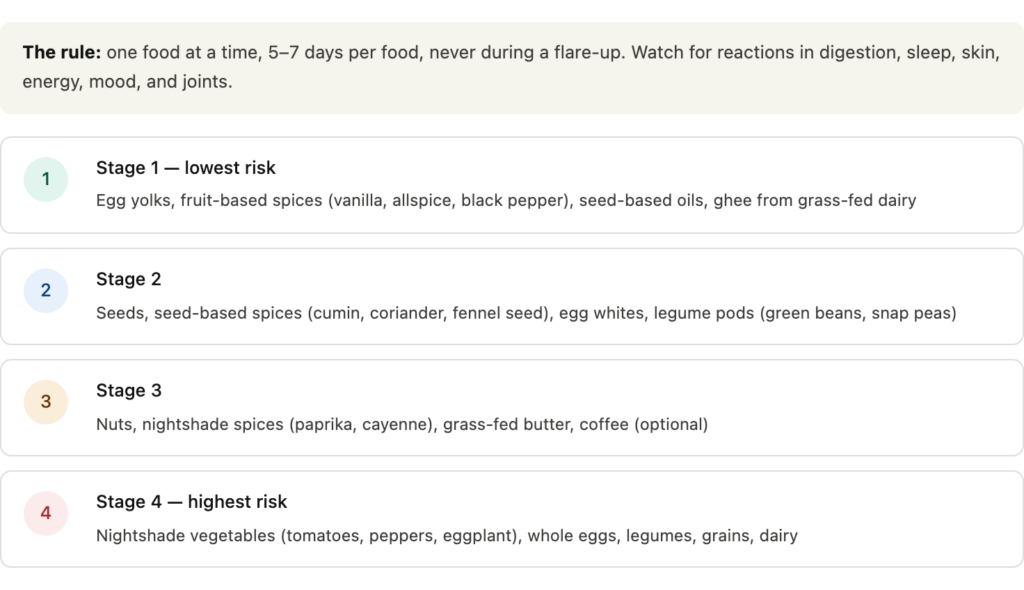
Reintroduction is where AIP becomes truly personalized. The protocol is methodical by design:
- Choose one food to reintroduce from the lowest-risk category.
- Consume a small amount on Day 1. If no reaction, a normal serving on Day 2.
- Wait 5–7 days observing for symptoms — digestive, skin, energy, mood, joint, sleep.
- If no reaction, the food is likely safe for you. If a reaction occurs, eliminate again and move on.
- Never reintroduce during a flare-up — baseline symptom control is required.
Reintroduction order matters. Lower-risk foods come first:
| Reintroduction stage | Foods |
| Stage 1 (lowest risk) | Egg yolks, fruit-based spices (pepper, vanilla), seed-based oils, ghee from grass-fed dairy |
| Stage 2 | Seeds, seed-based spices, egg whites, legume pods (green beans, peas) |
| Stage 3 | Nuts, nightshade spices (paprika, cumin), grass-fed butter |
| Stage 4 (highest risk) | Nightshade vegetables, eggs, legumes, grains, dairy |
Long-Term AIP: What It Actually Looks Like
AIP is not meant to be a permanent diet. Most people who complete elimination and reintroduction end up with a personalized version — typically a modified Paleo-style diet with specific individual exclusions based on their reintroduction results.
Some clients successfully reintroduce most foods. Others find that nightshades, eggs, or grains consistently trigger symptoms and choose to keep them out permanently. That’s the point — the protocol generates individual data that most generic elimination diets don’t.
Long-term AIP followers report that the most common permanent exclusions are: gluten-containing grains, nightshades (especially in Hashimoto’s clients), and dairy. These align with the foods most strongly associated with immune activation in the research literature.
AIP + Other Protocols: What Works and What Doesn’t
AIP + Low FODMAP
Short-term overlap can be useful for clients with concurrent SIBO or significant IBS alongside their autoimmune condition. The combination is highly restrictive and difficult to sustain — don’t recommend it for longer than 4–6 weeks without very close nutritional monitoring.
AIP + Wahls Protocol
Dr. Terry Wahls’ protocol for MS overlaps significantly with AIP and emphasizes many of the same principles. The two are compatible and many practitioners use Wahls as a long-term maintenance framework after AIP elimination.
AIP + Whole30
Whole30 is less restrictive than AIP (allows eggs, nightshades, most seeds). It can be a useful starting point for clients who find full AIP overwhelming, but it’s not a substitute for the full elimination if autoimmune triggers are the goal.
AIP and the Morning Ritual: What to Drink
Coffee is eliminated on AIP — it’s a common sticking point for clients, particularly those using coffee as a morning ritual that organizes their day. The good news: several AIP-compliant ingredients make excellent warm beverage alternatives.
Roasted chicory root, dandelion root, and carob are all AIP-compliant and produce a rich, coffee-like warm beverage when brewed. All three have clinical profiles relevant to autoimmune and gut health clients specifically:
- Chicory root — prebiotic inulin that feeds bifidobacteria; clinical trial data showing 3–4x bifidobacteria increase (Puhlmann et al., 2022). High FODMAP — use with caution in SIBO clients.
- Dandelion root — stimulates bile production and liver detoxification; taraxasterol provides hepatoprotective effects. SIBO-safe.
- Carob — SIBO-safe prebiotic fiber, D-pinitol for insulin sensitivity, condensed tannins with antimicrobial activity. Not high FODMAP.
If your clients want all three in a single AIP-compliant morning drink, Sip Herbals makes a roasted blend using all three ingredients. Caffeine-free, theobromine-free, and fits every AIP, Wahls, and anti-inflammatory protocol.
AIP Recipes to Get Your Clients Started
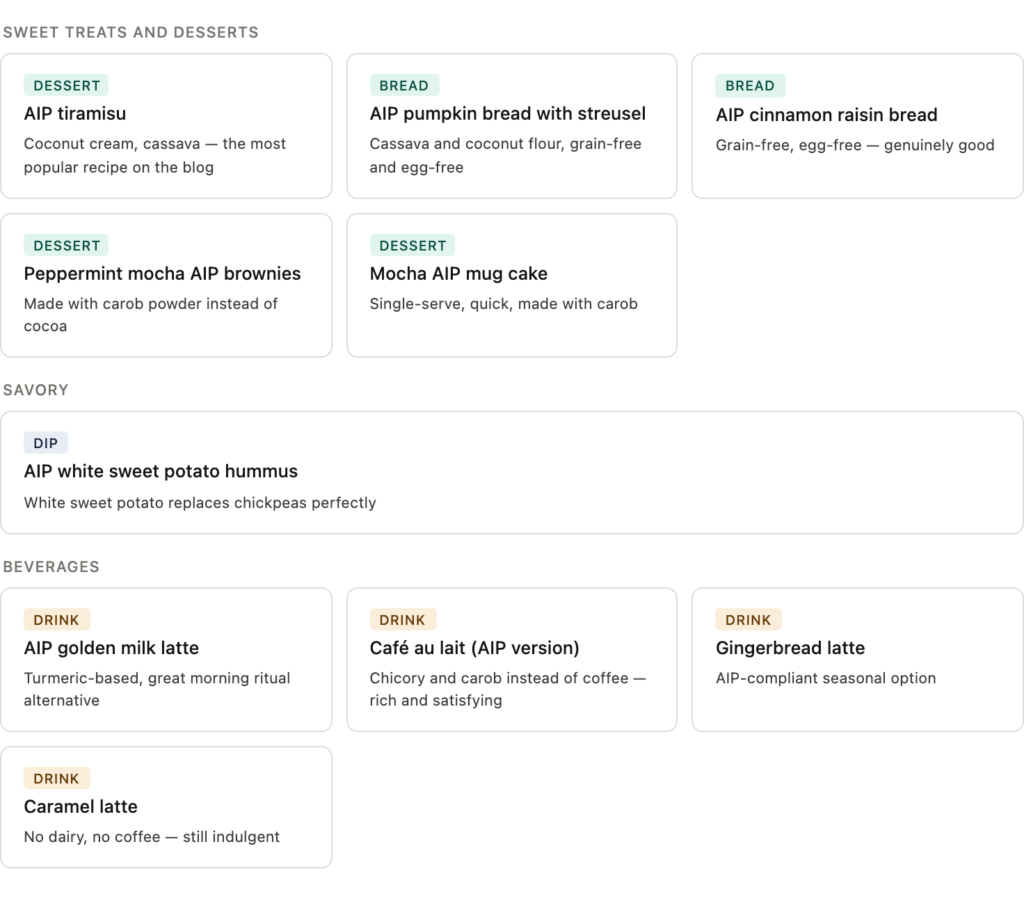
One of the biggest barriers to AIP is meal planning. Here are AIP-compliant recipes from our kitchen — all built around the elimination phase food list and tested to actually taste good:
Sweet treats and desserts
- AIP tiramisu — the most popular recipe on this blog for good reason. AIP-compliant, uses coconut cream and cassava.
- AIP pumpkin bread with streusel — perfect for fall, made with cassava and coconut flour.
- AIP cinnamon raisin bread — grain-free, egg-free, and genuinely good.
- Peppermint mocha AIP brownies — made with carob powder instead of cocoa.
- Mocha AIP mug cake — quick single-serve dessert using carob and Sip.
Savory and sides
- AIP golden milk latte — turmeric-based warm drink, great morning ritual alternative.
- AIP white sweet potato hummus — white sweet potato replaces chickpeas perfectly.
Beverages
- Café au lait (AIP version) — made with roasted chicory and carob instead of coffee.
- Gingerbread latte — AIP-compliant seasonal option.
- Caramel latte — no dairy, no coffee, still tastes indulgent.
Practical Tips for Clients Starting AIP
Before they start
- Clear the kitchen first — AIP is much harder when non-compliant foods are in the house.
- Batch cook a week’s worth of proteins and compliant vegetables before the first day.
- Stock compliant “rescue” snacks: plantain chips, cassava crackers, fruit, compliant jerky.
- Join a community — AIP Facebook groups, the Autoimmune Wellness website, and Mickey Trescott’s resources are excellent practical support.
During elimination
- Keep a symptom journal — track energy, digestion, sleep, skin, joint pain, mood. This data is essential for reintroduction.
- Don’t rush to reintroduce — 30 days minimum, 90 for complex or severe cases.
- Expect weeks 1–2 to be hard. Have them note the date they expect symptoms to ease.
- Bone broth daily supports gut lining repair — collagen, glycine, glutamine.
During reintroduction
- 5–7 days per food — not 1–2. Immune reactions can be delayed.
- Never reintroduce during a flare-up or period of high stress.
- One food at a time, always. Multiple reintroductions simultaneously make trigger identification impossible.
- Document everything — reactions can be subtle (mood shifts, sleep changes) as well as obvious.
When to Involve a Specialist
AIP is appropriate for many clients, but some situations call for additional professional oversight:
- Multiple autoimmune conditions — the interaction between conditions and dietary needs is complex.
- Active IBD with significant weight loss or nutritional deficiency risk.
- History of disordered eating — the restrictive nature of AIP can be triggering.
- No improvement after 90 days of strict elimination — may indicate other drivers beyond diet.
- On immunosuppressive medications — dietary changes can interact with medication efficacy.
Common Questions
How long does the elimination phase need to be?
Minimum 30 days. Most practitioners recommend 60–90 days for clients with chronic or severe autoimmune conditions. The IBD clinical data measured meaningful outcomes at week 6, but full gut healing takes longer. Don’t rush to reintroduce just because the minimum period is complete — the question is whether symptoms have stabilized, not just how many days have passed.
Is AIP safe long-term?
The elimination phase is not designed to be permanent. It’s restrictive enough that nutrient gaps are possible with prolonged elimination — particularly in fat-soluble vitamins if organ meats aren’t consumed regularly. The reintroduction phase exists precisely to move clients toward a more sustainable personalized diet. Long-term AIP looks more like a customized Paleo diet with individual exclusions than the full elimination protocol.
Can AIP help with Hashimoto’s?
The evidence shows symptom improvement and quality of life benefits, but not thyroid function normalization. A 10-week pilot study found improved symptom scores and reduced CRP, but no significant change in TSH or thyroid antibodies. Set this expectation clearly: AIP may help clients feel better and manage flare-ups, but it’s not a replacement for thyroid medication or a cure for the underlying condition.
Why are nightshades eliminated?
Nightshades (tomatoes, peppers, eggplant, potatoes) contain saponins — compounds that can increase intestinal permeability in susceptible individuals by disrupting cell membrane integrity. They also contain lectins and capsaicin, which can trigger immune responses. Not everyone reacts to nightshades, which is why they’re reintroduced systematically — many AIP clients successfully add them back without issue.
Is AIP the same as Paleo?
No — AIP is significantly more restrictive. Paleo allows eggs, nightshades, nuts, seeds, and seed-based oils. AIP eliminates all of these in the elimination phase. The reintroduction process is also absent from Paleo. AIP is best understood as an autoimmune-specific elimination diet built on a Paleo foundation.
What about coffee?
Coffee is eliminated on AIP. This is one of the most common client questions. The rationale: coffee is acidic, can increase cortisol, affects sleep architecture in ways that impair immune regulation, and — for clients on levothyroxine — binds to the medication and reduces absorption. AIP-compliant alternatives include roasted chicory root, dandelion root, and carob, all of which produce warm, coffee-like beverages without caffeine or theobromine.
How do I know if AIP is working?
The most reliable indicator is symptom tracking in a journal — not lab values, at least initially. Digestive improvement typically appears first (weeks 3–4). Joint pain, skin issues, and fatigue may take longer. Lab markers worth tracking at baseline and at 8–12 weeks: CRP, fecal calprotectin (for IBD), CBC, and condition-specific markers (TSH/TPO for Hashimoto’s, RF/anti-CCP for RA).
The Bottom Line
AIP is one of the most structured, evidence-informed dietary interventions available for autoimmune conditions. It’s not a miracle and it’s not appropriate for every client — but for the right population, with proper guidance and realistic expectations, it has a meaningful evidence base and a solid mechanistic rationale.
The clinical data supports its use most strongly for IBD and Hashimoto’s, with promising signals for RA. The reintroduction phase is what separates it from generic elimination diets — and it’s the part that actually makes the protocol useful long-term.
Help your clients understand that AIP is a reset, not a forever plan. The goal is to complete the protocol, gather individual data, and build a sustainable personalized diet that actually fits their life.
WANT THE FULL PROTOCOL Download The Anti-Inflammatory Morning Protocol — a free resource for practitioners working with gut and hormone clients. Includes a warm beverage comparison table, protocol-specific guidance, and client-ready language.
The Anti-Inflammatory Morning ProtocolSend download link to: |
References
1. Konijeti GG et al. Efficacy of the Autoimmune Protocol Diet for Inflammatory Bowel Disease. NCT03512327. Scripps Health. ClinicalTrials.gov
2. Abbott RD et al. Efficacy of the Autoimmune Protocol Diet as Part of a Multi-disciplinary, Supported Lifestyle Intervention for Hashimoto’s Thyroiditis. Cureus. 2019. PMC6592837
3. Ihnatowicz P et al. Effects of Autoimmune Protocol (AIP) diet on changes in thyroid parameters in Hashimoto’s disease. Ann Agric Environ Med. 2023. aaem.pl
4. Ballantyne S. The Paleo Approach. Victory Belt Publishing. 2014.
5. Autoimmune Protocol diet review. Examine.com
6. Autoimmune Wellness. AIP food list and reintroduction protocol. autoimmunewellness.com
Written by Orleatha Smith, Master Herbalist & Co-founder, Sip Herbals | Fact-checked by Last updated: April 2026

Orleatha Smith is a Master Herbalist and cofounder of Sip Herbals, with more than a decade serving the health and wellness community through science grounded, inclusive wellness education. She holds a Master’s Degree in Education, a biology teaching credential, and brings a rare mix of experience as a holistic lifestyle coach, SaaS developer, and organizational development specialist. Her work and insights have been featured in outlets including First for Women Magazine, The Los Angeles Times, and WebMD, alongside podcast and television appearances. Orleatha writes to help readers make practical, evidence informed wellness choices that fit real life.



